
Spectra Optia TPE vs. INUSpheresis: A Clinical Comparison of Therapeutic Plasma Exchange and Double Filtration Plasmapheresis


Patients researching advanced blood filtration for detoxification or autoimmune support frequently encounter two distinct therapies: Therapeutic Plasma Exchange (TPE) performed on the Spectra Optia system, and INUSpheresis, a European treatment based on Double Filtration Plasmapheresis (DFPP). A common assumption is that INUSpheresis represents the more advanced or selective option because it returns the patient's own filtered plasma. This article examines that assumption against the clinical evidence and explains why full-volume TPE remains the more comprehensive intervention for systemic detoxification and immune resetting.
How Therapeutic Plasma Exchange and INUSpheresis Differ
Both modalities process blood outside the body (apheresis) to remove harmful substances—including microplastics, mycotoxins, inflammatory exosomes, and autoantibodies. The fundamental distinction lies in what each does with the patient's plasma.
Spectra Optia TPE: Complete Plasma Replacement
Therapeutic Plasma Exchange on the Spectra Optia system performs wholesale removal. The procedure discards the patient's entire plasma volume and replaces it with pharmaceutical-grade donor albumin. Both harmful components (toxins, autoantibodies, inflammatory cytokines) and beneficial components (clotting factors, native albumin) are removed, and high-purity replacement fluid is infused in their place. The result is a complete reset of the plasma compartment.
INUSpheresis: Double Filtration Plasmapheresis
INUSpheresis is a form of Double Filtration Plasmapheresis (DFPP). It separates the plasma, passes it through a fine secondary filter to capture large molecules, and then returns the patient's own filtered plasma to circulation. The therapy is designed for the targeted removal of large molecules and relies on the reuse of the patient's existing proteins.
The perception that protein reuse is inherently advantageous is the central point worth scrutinizing.
The Albumin Binding-Capacity Advantage
Albumin is the primary transport protein in plasma, binding and carrying hormones, pharmaceuticals, and toxins throughout the body. Its detoxification value is determined by its binding capacity—the proportion of binding sites available to accept new molecules.
Fresh Donor Albumin Offers 100% Open Binding Capacity
Pharmaceutical donor albumin enters circulation with fully open binding capacity. Upon infusion, it immediately begins drawing toxins and metabolic waste out of the tissues, including stored burden that a single procedure could not otherwise reach. This post-procedure tissue redistribution is a meaningful therapeutic benefit of full plasma replacement.
Native Albumin May Be Saturated or Oxidatively Damaged
In patients carrying a significant toxic load, native albumin is often already saturated with bound compounds or damaged by oxidative stress. Because INUSpheresis returns the patient's own albumin, it may return protein with diminished capacity to support ongoing detoxification after the procedure. In this context, "retaining your own proteins" does not confer an advantage if those proteins can no longer bind effectively.
Additional Benefits of Full Plasma Replacement
Comprehensive cytokine removal: Replacing the entire plasma volume removes the broad burden of inflammatory signaling molecules rather than filtering for specific targets, substituting a clean, non-inflammatory fluid.
Antioxidant and vascular support: Fresh albumin exhibits antioxidant properties and helps stabilize the glycocalyx, the protective endothelial lining of the blood vessels.
Guaranteed purity of replacement fluid: Pharmaceutical albumin is highly purified and heat-treated, ensuring it is free of the microplastics, heavy metals, and environmental contaminants that may be present in native plasma.
Comparative Effectiveness: Toxin and Pathogen Removal
The following comparison summarizes how each modality performs across key target substances.
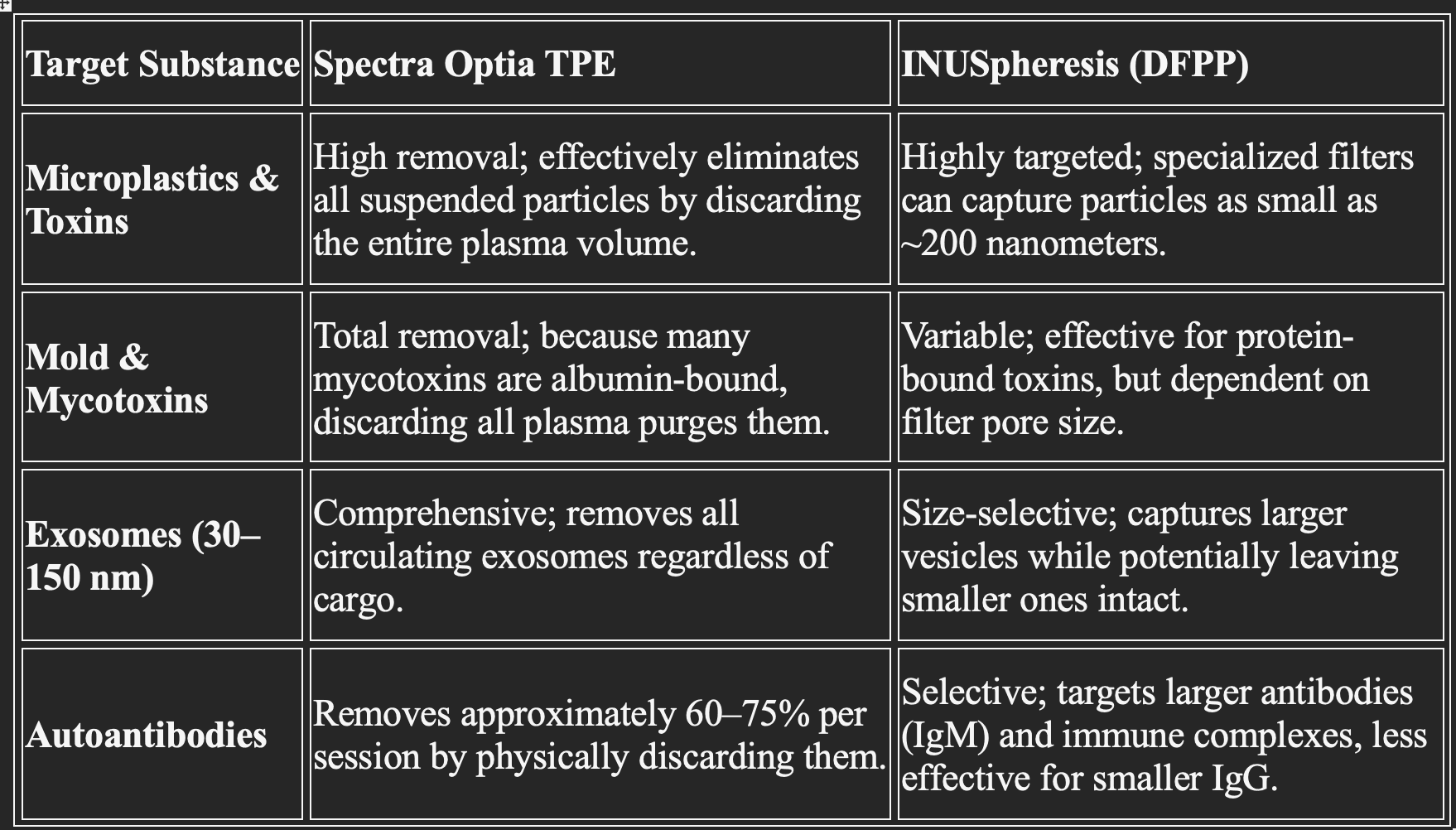
A consistent pattern emerges across these categories: INUSpheresis is selective by design. While selectivity is appropriate when removing a specific, known molecule, it functions as a constraint when the clinical objective is comprehensive removal of an unknown or heterogeneous burden.
Which Therapy Is Appropriate?
INUSpheresis (DFPP) is a capable therapy with legitimate applications, particularly where targeted removal of specific large molecules is the goal. However, when the objective is comprehensive systemic detoxification, reduction of a heavy inflammatory load, or restoration of albumin binding capacity, full-volume Therapeutic Plasma Exchange offers a more complete intervention. Rather than filtering and recycling the patient's existing plasma, TPE removes the problem entirely and restores a clean physiological foundation.
For this reason, 1.2 blood-volume TPE on the Spectra Optia system is widely regarded as the gold standard for systemic resetting.
Frequently Asked Questions
Is INUSpheresis better than TPE because it keeps my own proteins? Not necessarily. The benefit of native protein retention depends on whether that protein retains its binding capacity. In patients with a high toxic load, native albumin is often saturated or oxidatively damaged, whereas fresh donor albumin provides fully open binding capacity for continued detoxification.
Does Therapeutic Plasma Exchange remove microplastics and mycotoxins? Yes. Because TPE discards the entire plasma volume, it effectively removes suspended particles and albumin-bound toxins, including microplastics and many mycotoxins.
How much of circulating autoantibodies does TPE remove per session? Therapeutic Plasma Exchange removes approximately 60–75% of circulating autoantibodies per session by physically discarding the plasma in which they reside.